Claims rejected under CO 252 denial code often begin with a simple but frustrating question many billing teams search for: “Why was my claim denied for additional documentation even after submitting all required records?” In 2026, this issue remains common, as industry data shows that average initial claim denial rates range between 11% and 12%, meaning nearly 1 in 9 claims is denied on first submission due to documentation or coding gaps.
When healthcare providers or billing teams encounter the CO 252 denial code, the immediate challenge is delayed payment and additional administrative workload. Each denied claim increases rework cost, which industry benchmarks estimate at approximately $25–$30 per claim in administrative effort alone. Staff must pause claim processing to locate missing documents, validate coding, and resubmit corrected claims.
This section explains how the CO 252 denial code works, why it occurs, and how it affects billing performance. It also outlines both operational challenges and process-level opportunities. When analyzed correctly, CO 252 trends help billing teams identify documentation weaknesses, improve claim acceptance rates, and reduce repeat denials in future submissions.
CO 252 denial code in medical billing
The CO 252 denial code appears when a payer cannot process a claim due to missing or insufficient supporting documentation. This denial is common in hospital and physician billing workflows where attachments, clinical records, or authorization details are not fully submitted or validated at the time of claim submission.
From an operational view, CO 252 affects claim turnaround time, increases rework volume, and delays reimbursement cycles. It also signals gaps in documentation control, coding validation, or payer-specific submission requirements.
What CO 252 Denial Code Indicates
The CO 252 denial code indicates that the payer requires additional documentation before claim adjudication can continue. The claim is not rejected due to non-coverage alone but paused due to missing supporting evidence.
Key points linked to CO 252 include:
- Missing or incomplete clinical documentation
- Missing attachments such as reports, notes, or test results
- Lack of payer-required supporting evidence for medical necessity
- Incomplete submission of authorization or referral records
- Absence of required remark codes (RARC/NCPDP indicators)
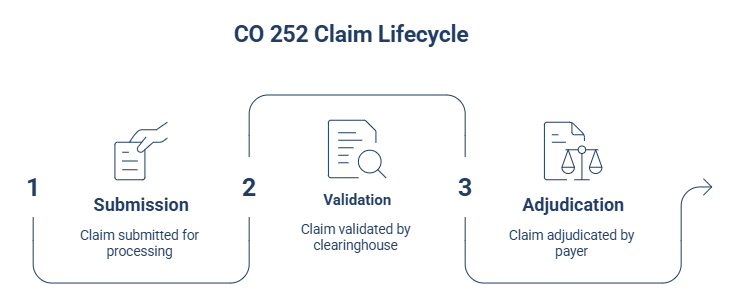
Where CO 252 Appears in Claim Lifecycle
The co 252 denial code can appear at multiple stages of the revenue cycle, depending on payer processing rules and submission method.
Typical points of occurrence include:
Claim submission stage: Initial claim lacks required attachments or supporting records
Clearinghouse validation stage: Missing electronic attachments or incomplete data trigger rejection signals
Payer adjudication stage: Payer requests additional documentation before final processing
Remittance stage: CO 252 is posted with remark codes identifying missing information
In electronic claim workflows, CO 252 is often linked with attachment validation failures where required supporting documents are not transmitted or not mapped correctly in the EDI transaction.
Key reasons behind the CO 252 denial code
From a revenue cycle perspective, CO 252 is not a single-point error. It is a result of multiple workflow gaps across documentation, coding, and authorization stages. Identifying the exact trigger is necessary to reduce repeat denials and avoid delays in reimbursement cycles.
Missing clinical or supporting documents
Missing clinical records remain the most common trigger for the CO-252 denial code. Payers require complete documentation to validate medical necessity and service accuracy.
Common missing elements include:
1. Physician progress notes
2. Operative or procedure reports
3. Diagnostic test results
4. Discharge summaries
5. Lab or imaging reports
Coding and claim entry errors
Coding inconsistencies directly contribute to the CO-252 denial code when claims fail documentation validation checks.
Frequent issues include:
1. Incorrect CPT or HCPCS codes
2. ICD-10 mismatch with documented diagnosis
3. Missing or invalid modifiers
4. Data entry errors in patient or service fields
Authorization and referral gaps
Authorization-related failures are another major cause of the CO-252 denial code. Many services require payer approval before delivery.
Key triggers include:
1. Missing prior authorization number
2. Referral not attached or invalid
3. Service performed outside authorized scope
4. Expired authorization at time of claim submission
Medical necessity gaps
Medical necessity issues arise when submitted documentation does not fully support the service billed, leading to co 252 denial code.
Common causes include:
1. Insufficient clinical justification in provider notes
2. Lack of documented patient condition severity
3. Missing evidence supporting treatment choice
4. Incomplete linkage between diagnosis and procedure codes
CO 252 denial code resolution steps
This section explains how billing teams, coders, and revenue cycle professionals should approach resolution in a controlled workflow. Each step focuses on identifying the missing element, correcting claim data, and ensuring documentation completeness before resubmission or escalation.
Review denial and remark codes
The first step in resolving co 252 denial code is reviewing the remittance advice in detail. Payers often attach remark codes that explain what documentation is missing or incomplete.
Key actions include:
- Identify CARC and RARC codes linked to the denial
- Check payer notes for specific documentation requests
- Confirm whether the issue is attachment-related or coding-related
- Determine if the claim is correctable or requires appeal
Collect missing documentation
Once the issue is identified, the next step is gathering all required records related to co 252 denial code.
Common documentation to collect:
- Clinical notes and provider documentation
- Diagnostic reports and lab results
- Procedure reports and operative notes
- Prior authorization or referral records
- Supporting medical necessity evidence
Correct claim and resubmit
After documentation is collected, the claim must be corrected before resubmission.
Key correction steps include:
- Validate CPT, ICD-10, and HCPCS coding accuracy
- Ensure patient demographics and insurance details are correct
- Attach all required supporting documentation
- Confirm payer-specific submission requirements are met
- Submit as a corrected claim through the clearinghouse
Appeal when required
If resubmission does not resolve the denial, escalation through the appeal process may be required.
Approach includes:
- Determine if payer requires formal appeal instead of correction
- Submit clinical justification with full documentation set
- Include provider notes supporting medical necessity
- Follow payer-specific appeal timelines and formats
- Track appeal status to avoid processing delays
Common remark codes linked with CO 252 denial code
The co 252 denial code is often posted with Remittance Advice Remark Codes (RARCs) that explain what specific documentation is missing. These remark codes are critical because they direct billing teams to the exact data required for claim processing. In 2026 claims processing workflows, payer systems increasingly rely on RARC pairing to reduce manual review, which makes correct interpretation essential for faster resolution.
Frequently attached RARC codes
The most common remark codes associated with co 252 denial code include the following:
| Remark Code | Meaning |
| N479 | Missing Explanation of Benefits (EOB) or coordination of benefits details |
| N710 | Missing clinical notes required for claim processing |
| N712 | Missing summary documentation for reviewed services |
| N714 | Missing diagnostic, lab, or assessment reports |
| N716 | Missing patient charts or supporting medical records |
How remark codes guide claim correction
Remark codes linked to co 252 denial code provide direct correction guidance for billing teams. They help identify what must be added before resubmission.
Key correction functions include:
- Identifying missing clinical or administrative documentation
- Reducing guesswork during claim correction
- Improving accuracy of resubmitted claims
- Supporting faster resolution in revenue cycle workflows
- Preventing repeated denial for the same issue
Conclusion
CO 252 denial code reflects a documentation-driven barrier in claim processing that directly impacts reimbursement timelines and billing efficiency. It highlights gaps in clinical records, coding accuracy, or required attachments that must be addressed before payer adjudication can continue.
A structured approach to review, correction, and resubmission helps reduce repeat denials and improves claim acceptance rates. Strengthening documentation practices and aligning with payer requirements supports a more stable and predictable revenue cycle.
FAQs
What does co 252 denial code mean in medical billing?
co 252 denial code means the payer needs additional documentation before processing the claim. It usually indicates missing attachments or incomplete supporting records required for adjudication.
What are the main causes of co 252 denial code?
Common causes include missing clinical documentation, coding errors, lack of prior authorization, missing referrals, and incomplete proof of medical necessity.
How can co 252 denial code be resolved quickly?
Review the remark codes, collect the missing documents, correct any claim errors, and resubmit the claim with complete and accurate supporting records.
Which documents are commonly required for co 252 denial code?
Required documents often include clinical notes, lab reports, imaging results, operative reports, discharge summaries, and authorization or referral records.
Can co 252 denial code be prevented in future claims?
Yes. It can be reduced by improving documentation processes, using claim scrubbing tools, training staff on payer rules, and verifying attachments before submission.