Are you submitting claims for injectable drugs and biologics but still facing denials despite accurate documentation? In 2026, billing errors related to HCPCS Level II codes, including J-codes, remain a top reason for claim rejections and delayed reimbursements. With 160 new codes added and 101 deleted from the HCPCS Level II list this year, providers who fail to update their coding may risk denied claims, lost revenue, and compliance issues.
J‑codes identify specific non‑oral medications and biologics that require precise dosage reporting and accurate reimbursement logic. Under Medicare Part B, most drug payments are based on Average Sales Price (ASP) + 6%, with national payment values published for commonly used codes. For instance, J0206 (allopurinol 1 mg) has a national Medicare reimbursement of approximately $4.40 per unit in 2026, making accurate coding critical to maintaining revenue flow.
This article explains how J‑codes function, why errors are costly, and how updated HCPCS requirements affect accurate drug coding, reimbursement, and compliance. It focuses on practical rules, payer expectations, and documentation essentials that matter to providers, coders, billers, and revenue cycle professionals.
What are The J-Codes: Know More About
This section explains the function, purpose, and application of J-Codes in medical billing. Understanding their role prevents errors and ensures proper reimbursement.
What are J codes
J-Codes are HCPCS Level II codes used for non-oral medications administered by healthcare professionals. They cover:
- Injectable drugs
- Biologics
- Chemotherapy medications
- Immunosuppressants
Why J-codes exist in HCPCS
J-Codes exist to standardize billing for drugs that cannot be self-administered orally. They allow:
- Consistent reporting across healthcare facilities and payers
- Accurate reimbursement under Medicare, Medicaid, and private insurers
- Clear documentation for regulatory compliance
- Streamlined revenue collection for specialty treatments
Where J-codes are used in healthcare billing
J-Codes are used primarily for claims submitted by:
- Oncology clinics (chemotherapy drugs)
- Hospitals and outpatient infusion centers
- Specialty practices administering biologics or immunosuppressants
- Emergency care and inpatient units for injectable treatments
HCPCS J Codes and Drug Classification
HCPCS J-Codes are a core component of J-Codes in Medical Billing. They separate medications, biologics, and injectable drugs from supply items. Misclassification can result in claim denials, delayed revenue, and compliance issues. In 2026, CMS reported that approximately 15% of Medicare Part B injectable drug claims required edits due to incorrect J-Code usage, emphasizing the need for accurate classification.
Medical J codes vs supply codes
Medical J-Codes represent drugs administered by healthcare professionals. In contrast, supply codes cover items like:
1. Infusion sets
2. Catheters
3. Needles and syringes
Key differences:
| Feature | J-Codes | Supply Codes |
| Represents | Drugs and biologics | Medical supplies |
| Billing Unit | Drug units, dosage | Each item or package |
| Reimbursement | Based on drug cost and HCPCS rules | Based on item cost |
J-codes for drugs and biologics
J-Codes cover a wide range of injectable medications, including:
| Category | Description | Example J-Codes | Notes for Billing |
| Chemotherapy Drugs | Medications used to treat cancer are often administered intravenously. | J9000–J9999 | Verify dose, units, and infusion documentation; apply JW/JZ modifiers for wastage. |
| Biologics | Complex proteins or monoclonal antibodies used for autoimmune, oncology, or rare disease treatment | J1300–J9999 | Requires NDC and ASP verification; check prior authorization and coverage. |
| Vaccines (Non-Preventive | Therapeutic vaccines are administered in clinical settings. | J1000–J1999 | Document lot numbers and NDC codes; confirm payer-specific rules. |
| Anti-infectives | IV antibiotics and antiviral therapies. | J0120–J0696 | Ensure units match dose administered; check coverage and medical necessity. |
| Anti-infectives | IV antibiotics and antiviral therapies. | J0120–J0696 | Ensure units match dose administered; check coverage and medical necessity. |
Temporary vs permanent J-codes
Permanent J-Codes: Established codes with ongoing coverage for frequently used drugs. Example: J9035 – bevacizumab 10 mg.
Temporary J-Codes (C-codes): Assigned to newly approved drugs before permanent assignment. Typically valid for two years while usage and pricing are evaluated. Example: J3490 – unclassified drugs.
J-Code Reimbursement and Payment Rules
J-Code reimbursement governs how healthcare providers receive payment for administering non-oral drugs. Inaccurate billing can lead to denials, delayed revenue, or compliance risks. According to CMS 2026 data, approximately 12–15% of injectable drug claims are edited or denied due to improper coding or misalignment with payment rules.
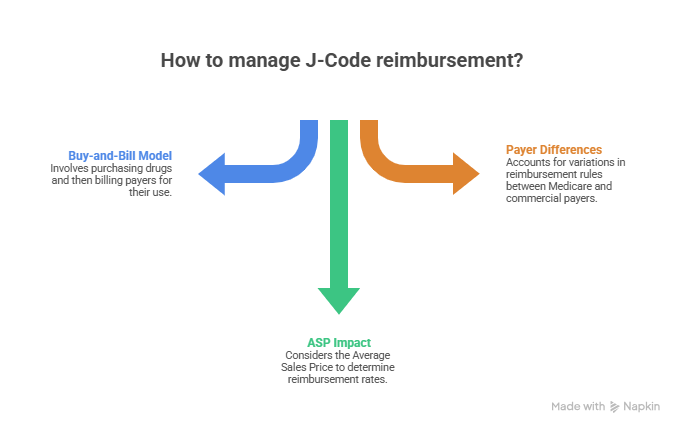
Buy-and-bill model
The buy-and-bill model is the standard for J-Code billing. Key points:
- Providers purchase the drug upfront.
- Medication is administered in the office or clinic.
- Provider submits a claim using the correct J-Code and units.
- Reimbursement covers drug cost plus an allowable administration fee.
Average Sales Price (ASP) impact
Medicare reimbursement for many J-Codes is tied to Average Sales Price (ASP):
- CMS sets payment at ASP + 6% for Part B drugs in 2026.
- ASP reflects the average cost of a drug across the U.S., updated quarterly.
- Correct ASP reporting is vital to avoid underpayment or overpayment recoupments.
Medicare vs commercial payer differences
Medicare reimburses based on HCPCS J-Codes, ASP, and fee schedules.
Commercial insurers may reimburse at contracted rates, sometimes higher or lower than Medicare.
Documentation, dosage, and administration details must align with payer policies to prevent denials.
J Code vs CPT Code
J-Codes and CPT codes serve different functions in medical billing. Misunderstanding their use can lead to rejected claims or delayed payments. In 2026, CMS data indicate that nearly 14% of injectable drug claims are flagged for coding errors due to improper J-Code and CPT code reporting. Providers, coders, and billing specialists must clearly distinguish the two to ensure correct reimbursement.
Purpose differences
J-Codes are used to report drugs and biologics administered by healthcare providers. They specifically identify the medication, dosage, and route of administration. This classification allows payers to track and reimburse drug costs accurately.
CPT codes, in contrast, report the procedures or services performed during the patient encounter. They document the administration of the drug, including infusion or injection services. Understanding the distinction is critical for accurate claims and compliance.
Reporting together on claims
Both J-Codes and CPT codes are submitted on the same claim to capture the full scope of patient care. J-Codes report the medication or biologic, while CPT codes indicate the administration service. This combination ensures transparency and correct payment.
Accurate reporting requires attention to units, modifiers, and administration notes. Claims with mismatched codes often result in denials or delayed reimbursement. Following payer guidelines reduces errors and speeds up revenue cycle processing.
Common pairing errors
Pairing errors often occur when J-Codes do not match the corresponding CPT codes. Other mistakes include reporting incorrect units or omitting necessary administration documentation. These errors are frequent in oncology, infusion, and specialty drug practices.
Incorrect pairings lead to claim denials, underpayment, or audit risks. Providers must verify coding accuracy before submission. Proper training and regular audits help prevent these common mistakes and safeguard practice revenue.
J-Codes for Chemotherapy Drugs
J-Codes for chemotherapy drugs are used to bill for cancer treatments based on the specific drug and dosage administered. Proper coding ensures accurate reimbursement, compliance with payer rules, and reduced risk of claim denials.
Oncology-Specific J-Codes
Chemotherapy billing carries a higher risk for errors due to complex protocols and multiple drug combinations.
| J-Code | Drug / Biologic | Route & Use | Billing Notes |
| J9355 | Bortezomib | IV/Subcutaneous; multiple myeloma | Dose-based billing; verify patient weight. Use JW/JZ modifier for wastage. |
| J9267 | Paclitaxel | IV infusion; various cancers | Ensure infusion records match units billed. Document lot numbers. |
| J9305 | Rituximab | IV: lymphoma, leukemia | Prior authorization is often required. Track infusion date and dose. |
| J9310 | Trastuzumab | IV: breast cancer, gastric cancer | Correct dose and frequency critical for reimbursement. |
| J9350 | Lenalidomide | Oral; multiple myeloma | Billing may require NDC reporting. Confirm prescription and patient adherence. |
| J9177 | Fluorouracil | IV: colorectal, breast cancer | IV: colorectal, breast cancer |
| J9312 | Bevacizumab | IV: colorectal, lung, kidney cancers | Documentation of dose, wastage, and prior authorization is mandatory. |
Dose-based billing rules
J-Codes for chemotherapy are typically billed based on the actual dosage administered. Accurate calculation of units according to milligrams, milliliters, or vials is required for correct reimbursement. Providers must cross-check patient charts against drug administration logs.
Incorrect dosage reporting can lead to underpayment or claim rejection. Following payer-specific rules ensures claims reflect true drug usage. Standardized templates and software checks help maintain billing accuracy and compliance.
Wastage and JW/JZ Modifiers
| Modifier | Purpose | When to Use |
| JW | Reports the discarded drug amount | When a portion of a single-dose vial is not administered and must be wasted |
| JZ | Confirms no drug wastage | When the entire amount of a single-dose vial is used |
| No Modifier | Not acceptable (2026 CMS rules) | Claims missing JW or JZ for single-dose vials |
| Single-Dose Vials | JW/JZ applicable | Medicare and many commercial payers require reporting |
| Multi-Dose Vials | JW/JZ not allowed | Drugs designed for multiple uses |
| Audit Risk Area | High scrutiny | Oncology and high-cost biologics |
Common J-Code Billing Errors and Denials
J-code billing errors are a leading cause of claim denials and delayed reimbursements in 2026. Many practices reduce recurring claim rejections by implementing structured Denial Management Services that identify coding and reimbursement issues before claims are resubmitted. Common mistakes include mismatched units, missing NDC information, and gaps in coverage or prior authorization.
Units mismatch
Unit mismatches occur when the number of J-code units billed does not match the actual quantity administered. This can lead to claim denials, delayed payments, and potential audits. Providers must verify dose documentation and compare it with the units billed.
Incorrect unit reporting is frequent in oncology and specialty drug administration. Consistently reviewing infusion logs and medication orders ensures accuracy and reduces payer rejections.
Missing NDC data
Many claims are denied due to absent or incorrect National Drug Code (NDC) information. NDC reporting is essential for accurate drug identification, pricing, and reimbursement.
Medical billing teams should cross-check the drug’s NDC in the patient’s chart against the claim form. Using outdated or invalid NDCs can trigger denials from Medicare and commercial payers.
Coverage and authorization gaps
J-code denials often arise when pre-authorization or coverage requirements are incomplete. Payers require documentation confirming medical necessity before approving high-cost drugs.
Practice managers and billing specialists must verify insurance eligibility, confirm prior authorizations, and maintain proper documentation. Accurate verification processes supported by professional Medical Billing Services can help reduce authorization-related claim issues and improve reimbursement timelines. Proactive checks prevent claim rejections and accelerate reimbursement cycles.
Conclusion
Accurate J-Code reporting directly affects reimbursement accuracy, audit exposure, and regulatory standing for drug and biologic claims. Consistent alignment between documentation, dosage, NDC data, and payer rules supports payment stability across Medicare and commercial plans.
Providers, coders, and billing teams that apply current HCPCS guidance, verify units, and confirm authorization requirements reduce preventable denials. Strong internal review practices help protect revenue integrity while meeting 2026 compliance expectations.
FAQs
What are J-Codes in Medical Billing used for?
J-Codes in Medical Billing identify non-oral drugs and biologics administered by healthcare providers. They support accurate drug reporting, pricing, and payer reimbursement.
How are J-Codes reimbursed under Medicare in 2026?
Most Medicare Part B J-Codes are paid at Average Sales Price (ASP) plus 6%.
Rates are updated quarterly, making current coding and unit accuracy essential.
Why do J-Code claims get denied despite correct documentation?
Denials often occur due to unit mismatches, missing NDC data, or absent authorization.
Even minor reporting gaps can trigger claim edits or payment delays.
What is the difference between J-Codes and CPT codes?
J-Codes report the drug or biologic administered during care. CPT codes report the injection or infusion service provided.
When are JW and JZ modifiers required for J-Code billing?
JW reports discarded drug from single-dose vials, while JZ confirms no wastage.
CMS requires one of these modifiers on applicable claims in 2026.