Medical coding is more than just assigning codes to diagnoses and procedures. It directly affects hospital revenue, claim approvals, compliance, and even patient outcomes. One of the most important distinctions every coder, healthcare provider, and billing professional must understand is the difference between inpatient coding and outpatient coding.
At first glance, both may seem similar since they rely on standardized coding systems and clinical documentation. However, the reality is far more nuanced. The rules, complexity, reimbursement models, and even the level of expertise required can differ significantly. A small misunderstanding in these areas can lead to claim denials, revenue loss, or compliance issues.
Whether you are a beginner exploring a career in medical coding, a professional aiming to sharpen your skills, or a healthcare organization looking to improve billing accuracy, understanding these differences is essential. This article breaks down inpatient coding and outpatient coding in a clear, practical, and detailed way so you can confidently apply the right approach in real-world scenarios.
What is Medical Coding?
Medical coding is the process of translating healthcare diagnoses, procedures, services, and equipment into standardized alphanumeric codes. These codes are derived from clinical documentation such as physician notes, lab reports, and discharge summaries. They play a critical role in the healthcare ecosystem by ensuring that providers are accurately reimbursed and that patient records are consistently maintained.
At its core, medical coding acts as a bridge between healthcare providers and insurance companies. Without accurate coding, claims can be delayed, denied, or underpaid. This makes coding not just an administrative task, but a revenue-critical function.
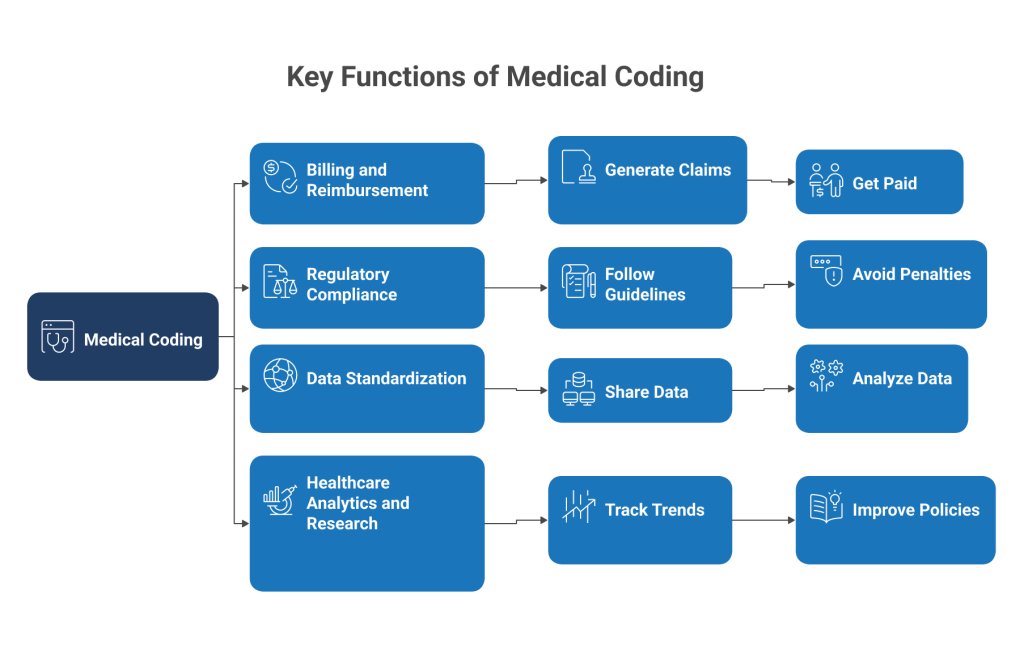
Key Functions of Medical Coding
- Billing and Reimbursement
Codes are used to generate claims submitted to insurance companies. Accurate coding ensures healthcare providers are paid correctly for their services. - Regulatory Compliance
Medical coding must follow strict guidelines set by organizations such as CMS and WHO. Incorrect coding can lead to audits and penalties. - Data Standardization
Coding creates a universal language that allows healthcare data to be shared and analyzed across systems. - Healthcare Analytics and Research
Coded data is used to track disease trends, measure outcomes, and improve healthcare policies.
Common Coding Systems Used
- ICD-10-CM: Used for diagnosis coding in both inpatient and outpatient settings.
- ICD-10-PCS: Used for inpatient procedure coding, especially in hospital settings.
- CPT Codes: Used primarily in outpatient settings to describe medical procedures and services.
- HCPCS Codes: Used for additional services such as medical equipment and supplies.
Understanding these coding systems is essential before diving into the differences between inpatient and outpatient coding, as each setting uses them differently based on the type of care provided.
What is Inpatient Coding?
Inpatient coding refers to the process of assigning codes for patients who are formally admitted to a hospital for treatment, typically for more than 24 hours. These cases often involve complex medical conditions, multiple procedures, and extended stays, making inpatient coding one of the most detailed and challenging areas in medical coding.
Unlike outpatient coding, inpatient coding requires a comprehensive review of the entire patient stay, from admission to discharge. Coders must analyze all relevant documentation to determine the correct diagnoses and procedures while adhering to strict coding guidelines.
Key Characteristics of Inpatient Coding
- Admission-Based Care
Patients are admitted to the hospital for ongoing treatment, monitoring, or surgery. - Complex Medical Cases
Cases often involve multiple diagnoses, comorbidities, and complications that must be accurately captured. - Extended Length of Stay
Patients typically remain in the hospital for more than a day, sometimes for weeks depending on the severity of the condition. - Comprehensive Documentation Review
Coders must review discharge summaries, physician notes, operative reports, lab results, and imaging studies.
Coding Systems Used in Inpatient Settings
- ICD-10-CM (Diagnosis Coding): Used to identify the patient’s primary condition and any secondary diagnoses.
- ICD-10-PCS (Procedure Coding): Specifically designed for inpatient procedures, providing detailed information about surgical and medical interventions.
Important Concepts in Inpatient Coding
Principal Diagnosis
The principal diagnosis is the main condition responsible for the patient’s admission to the hospital. Selecting the correct principal diagnosis is critical because it directly impacts reimbursement and clinical reporting.
MS-DRG Reimbursement System
Inpatient coding uses the Medicare Severity Diagnosis Related Group system, which determines how much a hospital is paid based on the patient’s diagnoses and procedures.
- Payment is fixed per case rather than per service
- More complex cases typically result in higher reimbursement
- Accurate coding ensures proper grouping and payment
Why Inpatient Coding is More Complex
- Multiple conditions must be sequenced correctly
- Coders must interpret detailed clinical documentation
- Guidelines are stricter and more nuanced
- Errors can significantly impact hospital revenue
Inpatient coding requires a deep understanding of medical terminology, anatomy, and coding guidelines. It is often considered more advanced compared to outpatient coding due to the level of detail and responsibility involved.
What is Outpatient Coding?
Outpatient coding refers to the process of assigning medical codes for patients who receive care without being admitted to the hospital. These services are typically completed within the same day, and the patient is discharged shortly after treatment. Outpatient coding is commonly used in clinics, emergency departments, ambulatory surgery centers, and diagnostic facilities.
While outpatient coding is generally less complex than inpatient coding, it still requires a high level of accuracy. Coders must focus on the specific services provided during the visit and ensure that each procedure and diagnosis is properly documented and coded.
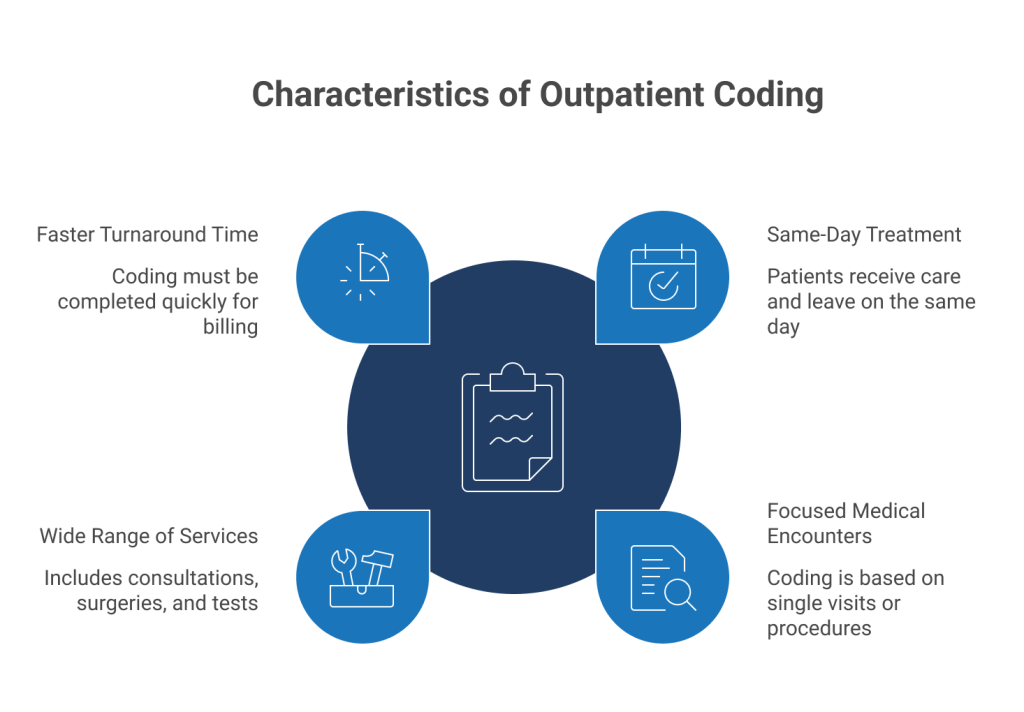
Key Characteristics of Outpatient Coding
Same-Day Treatment: Patients receive care and leave the facility on the same day without formal admission.
Focused Medical Encounters: Coding is based on a single visit or procedure rather than an extended stay.
Wide Range of Services: Includes consultations, minor surgeries, diagnostic tests, and emergency care.
Faster Turnaround Time: Coding must often be completed quickly to support timely billing and reimbursement.
Coding Systems Used in Outpatient Settings
- ICD-10-CM (Diagnosis Coding): Used to document the reason for the visit and any confirmed conditions.
- CPT Codes (Current Procedural Terminology): Used to describe medical, surgical, and diagnostic services performed.
- HCPCS Codes: Used for additional services such as medical supplies, equipment, and certain medications.
Important Concepts in Outpatient Coding
First-Listed Diagnosis
In outpatient coding, the first-listed diagnosis is the main reason for the patient’s visit. Unlike inpatient coding, uncertain diagnoses are not coded. Instead, symptoms and signs are reported if a definitive diagnosis has not been established.
APC Reimbursement System
Outpatient services are reimbursed using the Ambulatory Payment Classification system.
- Payment is based on individual services provided
- Each procedure or service is assigned a specific payment rate
- Multiple services may be billed for a single visit
Why Accuracy Matters in Outpatient Coding
- Incorrect procedure coding can lead to underpayment or overbilling
- Missing codes can result in claim denials
- Compliance errors can trigger audits
Even though outpatient coding may seem straightforward, the need for precision and speed makes it equally demanding in a different way.
Inpatient Coding vs Outpatient Coding
Understanding the core differences between inpatient and outpatient coding is essential for anyone working in healthcare billing or coding. The comparison below highlights how these two coding types differ across key areas.
| Feature | Inpatient Coding | Outpatient Coding |
| Patient Stay | Admitted for extended care | Treated and discharged the same day |
| Coding Systems | ICD-10-CM and ICD-10-PCS | ICD-10-CM, CPT, HCPCS |
| Reimbursement Model | MS-DRG (case-based) | APC (service-based) |
| Complexity Level | High due to multiple conditions | Moderate and focused |
| Documentation | Detailed and comprehensive | Specific to the visit |
| Diagnosis Selection | Principal diagnosis | First-listed diagnosis |
Key Differences Between Inpatient and Outpatient Coding
While both inpatient and outpatient coding serve the same ultimate purpose, which is accurate documentation and reimbursement, the way they operate in practice is very different. These differences influence everything from daily workflow to required expertise and financial outcomes.
Coding Systems
One of the most fundamental differences lies in the coding systems used for procedures.
Inpatient Coding: Uses ICD-10-PCS for procedures, which is highly detailed and structured. Each code reflects specific aspects such as approach, body part, and device used.
Outpatient Coding: Uses CPT and HCPCS codes, which are more service-oriented and widely used for physician and clinical procedures.
This difference means inpatient coders must have a deeper understanding of procedural details, while outpatient coders focus more on service classification.
Documentation Requirements
Documentation plays a crucial role in both coding types, but the depth and scope vary significantly.
Inpatient Coding: Requires a complete review of the patient’s entire stay, including:
- Admission notes
- Progress notes
- Operative reports
- Discharge summaries
- Lab and imaging results
Outpatient Coding
Focuses only on documentation related to the specific visit or procedure:
- Physician notes
- Procedure reports
- Diagnostic findings
Inpatient coding demands a broader clinical perspective, while outpatient coding requires precise interpretation of a single encounter.
Diagnosis Coding Rules
The way diagnoses are selected and reported differs between the two settings.
- Inpatient Coding
- Uses the principal diagnosis, which is the condition responsible for admission
- Can code confirmed diagnoses even if established after study
- Outpatient Coding
- Uses the first-listed diagnosis, which is the reason for the visit
- Does not allow coding of suspected conditions
- Symptoms are coded when no confirmed diagnosis is available
These rules directly impact coding accuracy and compliance.
Reimbursement Models
The payment structure is another major distinction that affects how coding is approached.
- Inpatient Coding
- Uses MS-DRG system
- Payment is fixed per case
- Severity and complications increase reimbursement
- Outpatient Coding
- Uses APC system
- Payment is based on each individual service
- Multiple procedures can generate multiple payments
This makes inpatient coding more outcome-focused, while outpatient coding is service-driven.
Complexity Level
The level of difficulty varies due to the nature of patient care.
- Inpatient Coding
- Involves multiple diagnoses and procedures
- Requires advanced clinical knowledge
- Higher risk of errors impacting large payments
- Outpatient Coding
- Usually involves fewer diagnoses
- Faster coding turnaround
- Requires strong attention to detail for accuracy
Workflow and Time Requirements
- Inpatient Coding
- Longer time required per case
- Requires analysis of full patient history during stay
- Outpatient Coding
- Faster processing due to shorter encounters
- Often handled in high volumes daily
Similarities Between Inpatient and Outpatient Coding
Despite their differences, inpatient and outpatient coding share several core principles. These similarities ensure consistency across the healthcare system and maintain standardization in reporting and billing.
Shared Foundations
Use of ICD-10-CM for Diagnosis Coding: Both inpatient and outpatient settings rely on ICD-10-CM to document patient conditions accurately.
Dependence on Clinical Documentation: Accurate coding in both settings depends entirely on clear, complete, and detailed medical records.
Compliance with Regulatory Guidelines: Coders in both areas must follow official coding guidelines and payer-specific rules to avoid penalties and audits.
Role in Revenue Cycle Management: Coding directly impacts billing, reimbursement, and overall financial performance of healthcare organizations.
Shared Goals
- Accuracy in Reporting: Ensuring that diagnoses and procedures are correctly represented.
- Minimizing Claim Denials: Proper coding reduces the chances of rejected or delayed claims.
- Maintaining Compliance: Adhering to healthcare laws and coding standards is critical in both settings.
- Supporting Patient Care Data: Coded data helps improve treatment outcomes and healthcare analytics.
Common Skills Required
Both inpatient and outpatient coders need a strong foundation in:
- Medical terminology
- Anatomy and physiology
- Attention to detail
- Analytical thinking
- Knowledge of coding guidelines
Even though the application differs, the core skill set overlaps significantly.
Common Challenges in Inpatient vs Outpatient Coding
Even experienced coders face challenges when working with inpatient and outpatient records. These challenges can affect accuracy, compliance, and reimbursement if not handled properly.
Documentation Gaps
Incomplete or unclear documentation is one of the biggest issues in medical coding.
- Missing details about procedures or diagnoses
- Lack of physician clarification
- Inconsistent terminology across records
In inpatient coding, this becomes more critical because multiple providers are involved. In outpatient coding, even a small missing detail can lead to incorrect procedure coding.
Coding Errors and Claim Denials
Errors in coding can directly impact revenue and operational efficiency.
- Incorrect code selection
- Wrong sequencing of diagnoses
- Missing modifiers in outpatient procedures
These mistakes often result in:
- Claim rejections
- Payment delays
- Revenue loss
Constantly Changing Regulations
Medical coding guidelines are frequently updated, which makes it challenging to stay current.
- Updates in ICD-10 codes
- Changes in CPT and HCPCS codes
- New payer policies and compliance rules
Coders must continuously learn and adapt to avoid compliance risks.
Complexity in Inpatient Records
Inpatient coding involves reviewing extensive patient data, which increases the difficulty level.
- Multiple comorbidities and complications
- Long hospital stays with evolving diagnoses
- Complex surgical procedures
This requires strong analytical skills and deep clinical understanding.
Time Pressure in Outpatient Coding
Outpatient coding often involves high volumes and tight deadlines.
- Quick turnaround requirements
- Large number of daily cases
- Need for speed without compromising accuracy
Balancing speed and precision is one of the biggest challenges in outpatient settings.
Career Opportunities in Inpatient vs Outpatient Coding
Medical coding offers diverse career paths, and understanding the difference between inpatient and outpatient coding can help you choose the right specialization based on your skills and goals.
1. Skills Required for Inpatient Coding
Inpatient coding is considered more advanced and requires a deeper level of expertise.
- Strong understanding of anatomy, physiology, and disease processes
- Ability to analyze complex medical records
- Knowledge of ICD-10-PCS coding system
- Critical thinking and attention to detail
- Familiarity with MS-DRG reimbursement
Because of its complexity, inpatient coding roles often require more experience and specialized training.
2. Skills Required for Outpatient Coding
Outpatient coding focuses more on speed, accuracy, and handling volume.
- Proficiency in CPT and HCPCS codes
- Ability to code quickly without errors
- Understanding of modifiers and billing rules
- Attention to detail for single-visit encounters
- Time management skills
Outpatient coding is often a great entry point for beginners in the coding field.
3. Certifications to Consider
Certifications play a major role in advancing your career in medical coding.
- CPC (Certified Professional Coder): Ideal for outpatient coding and physician-based settings
- CCS (Certified Coding Specialist): Highly valued for inpatient coding roles
- RHIT (Registered Health Information Technician): Covers both inpatient and outpatient coding knowledge
- CCA (Certified Coding Associate): Entry-level certification for beginners
Choosing the right certification depends on whether you want to specialize in inpatient or outpatient coding.
Conclusion
Inpatient and outpatient coding may seem similar at a surface level, but they differ significantly in complexity, coding systems, documentation requirements, and reimbursement models. Understanding these differences is essential for accurate coding, compliance, and financial success in healthcare.
Inpatient coding demands deep clinical knowledge and careful analysis of complete patient records, making it a more advanced specialization. Outpatient coding, on the other hand, focuses on speed, precision, and handling a high volume of cases efficiently.