Have you ever thought why a provider engaged three months ago may still not be seeing patients, and whether that delay is costing your practice money? In 2026, research of more than 580 healthcare leaders 69% of hospitals and provider groups reported losing $1,000-$5,000 per provider per day due to credentialing constraints that slowed enrollment and patient treatment. Many organizations claim annual losses of more than $1 million due to weak credentialing.
Delegated credentialing becomes a key issue when accountability is uncertain. Many healthcare organizations believe that when credentialing is outsourced, risk and oversight also move. This assumption causes compliance gaps, NPDB breaches, payer audits, and delayed or rejected claims. According to a 2026 industry survey, approximately one-third of firms attribute 25%-50% of denials to payer registration problems, highlighting the impact of inefficient credentialing on revenue cycles and billing performance.
A detailed explanation is needed for providers, credentialing specialists, and billing teams to understand delegated credentialing, its differences from non-delegated models, and where responsibility is fixed.
This blog explains the contrasts, demonstrates how they impact compliance and revenue cycle outcomes, and highlights where delegated credentialing improves operational efficiency while introducing financial and regulatory risk.
Delegated Credentialing
This section explains what delegated credentialing is, its regulatory basis, and where accountability resides. You will understand authority transfer, NPDB rules, and legal exposure.
What Is Delegated Credentialing?
Delegated credentialing is when one healthcare entity gives another entity authority to carry out credentialing tasks. The delegated entity verifies professional qualifications, state licensing, board certifications, work history, sanctions, and other credentialing data. The intent is to shorten approval time and support payer enrollment. The delegating organization signs an agreement that defines what tasks are transferred and what obligations remain. This authority transfer affects reporting, oversight, and decision documentation.
Regulatory Foundation and NPDB Rules
The National Practitioner Data Bank (NPDB) establishes strict guidelines for delegated credentialing activity. Only the entity with credentialing authority may query the NPDB and use the results for decision-making. A delegating payer cannot receive NPDB responses from a query run under delegation. Hospitals or provider groups acting as delegates must submit NPDB queries themselves or through an authorized agent. Any attempt to share NPDB data outside the credentialing decision pathway violates federal policy and may trigger audit findings.
Credentialing, Accountability, and Legal Exposure
Delegated credentialing transfers operational tasks but does not transfer ultimate legal responsibility. The delegating entity remains accountable for compliance with payer agreements, standards such as those from the National Committee for Quality Assurance, and audit outcomes. Failure to meet verification requirements or reporting timelines can result in delegation loss, contracted penalties, or provider network disruptions. Credentialing and billing staff must maintain complete documentation and align credentialing files with payer and regulatory timelines to protect revenue and legal standing.
What Is Delegated Credentialing vs Non-Delegated Credentialing
This section compares delegated and non-delegated credentialing. It highlights operational differences, responsibilities, and the impact on provider onboarding, billing, and compliance.
Delegated Credentialing
Delegated credentialing allows a healthcare organization to transfer credentialing tasks to a qualified entity. The delegated entity verifies licenses, board certifications, work and malpractice history, and other professional credentials. The process shortens approval timelines and enables providers to join payer networks faster. Responsibilities and reporting requirements are clearly defined in a delegated credentialing agreement. This arrangement reduces administrative workload for payers and accelerates revenue cycle processes.
Key Points:
- The delegated entity performs primary source verification.
- Provider enrollment can occur in bulk.
- Delegating entity remains legally responsible for compliance.
- Timelines are generally faster, often completed within 4–6 weeks.
Non-Delegated Credentialing
Non-delegated credentialing occurs when the payer manages the entire credentialing process. Providers submit credentials individually to the insurer. This method is common for smaller practices with limited staff or infrastructure. Approval and network inclusion timelines are longer, often 90–120 days. This increases risk for claim delays and impacts cash flow. Administrative work remains with the payer, but providers may face repeated verification requests if they work with multiple payers.
Key Points:
- Payer conducts all credentialing and verification.
- Processing times are slower, typically exceeding 90 days.
- Limited administrative responsibility for providers, but revenue may be delayed.
- Compliance is managed entirely by the payer.
Key Differences Between Delegated and Non-Delegated Credentialing
Here are the key factors that differentiate the delegated and non-delegated credentialing.
| Factor | Delegated Credentialing | Non-Delegated Credentialing |
| Authority | The delegated entity conducts verification | Payer performs verification |
| Timeline | Faster, often 4–6 weeks | Slower, 90–120 days |
| Accountability | Delegating entity responsible for compliance | Payer responsible |
| Administrative Load | Reduced for payers, increased for delegated ent | Minimal for providers, high for payers |
| Revenue Impact | Accelerates claims and reimbursement | Potential delays in billing |
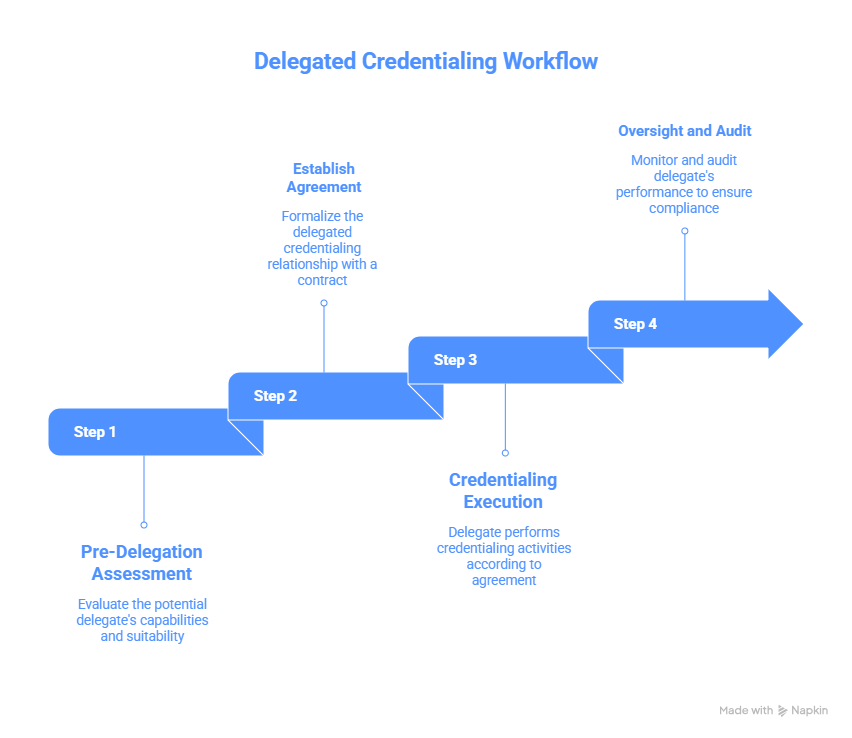
Delegated Credentialing Workflow
This section explains the step-by-step workflow for delegated credentialing. It highlights tasks, responsibilities, and timelines to ensure compliance and faster provider enrollment.
Step 1:Pre-Delegation Assessment
Before any delegation, healthcare organizations must audit their policies and systems. Evaluate staffing, software, and verification procedures against NCQA, CMS, or payer standards. Identify gaps in credentialing and quality oversight. This ensures the organization meets regulatory requirements and can manage delegated tasks without risk.
Key Points:
- Audit policies and procedures for compliance.
- Review credentialing staff capacity and software tools.
- Identify gaps in provider verification processes.
- Establish quality oversight metrics for delegated entities.
Step 2: Establish Delegated Credentialing Agreement
A formal agreement must be in place before delegation begins. The agreement clearly defines responsibilities, reporting schedules, audit requirements, and compliance expectations. Both delegating and delegated entities must sign the contract to enforce accountability.
Key Points:
- Outline delegated tasks and responsibilities.
- Define reporting formats and timelines.
- Specify audit schedules and compliance monitoring.
- Include termination clauses and regulatory adherence requirements.
Step 3: Credentialing Execution
The delegated entity conducts verification for provider licensure, DEA registration, board certifications, work and malpractice history, and hospital affiliations. All data is verified against primary sources. The delegated entity submits provider rosters and credentialing reports to the delegating organization and payers within agreed timelines.
Key Points:
- Verify licenses, DEA, board certifications, and affiliations.
- Conduct primary source verification for all providers.
- Maintain accurate, up-to-date credentialing files.
- Submit reports to the delegating entity and payer per agreement.
Step 4: Oversight and Audit
The delegating organization remains responsible for compliance. Annual audits by NCQA, CMS, or payers are conducted to verify adherence to credentialing standards. Discrepancies are addressed promptly to prevent delays in provider onboarding and reimbursement.
Key Points:
- Conduct annual oversight audits.
- Review credentialing files and compliance records.
- Correct non-compliance issues promptly.
- Ensure adherence to federal, state, and payer requirements.
Compliance Risks in Delegated Credentialing
This section highlights the key compliance risks associated with delegated credentialing. It explains how errors can impact audits, revenue, and provider liability.
H3: Regulatory Compliance Challenges
Delegated credentialing shifts responsibility to the provider organization, but oversight remains critical. Failure to follow NCQA, CMS, or payer rules can trigger fines, audits, or delayed reimbursements.
Key Points:
- Non-compliance with NCQA or CMS guidelines increases audit risk.
- Inaccurate provider data can lead to claim denials.
- Missing licensure or DEA verification exposes legal liability.
Audit and Reporting Obligations
Delegated entities must maintain accurate documentation and submit reports on time. Delayed or incomplete reporting can result in penalties, contract terminations, and delayed provider onboarding.
Key Points:
- Maintain credentialing logs for all providers.
- Submit timely reports to payers and delegating entities.
- Track audit findings and implement corrective actions.
Legal Exposure and Liability
Even when delegated, the contracting healthcare organization retains ultimate responsibility. Mistakes in credentialing can lead to legal action, reimbursement disputes, or regulatory penalties.
Key Points:
- The delegating organization remains accountable for credentialing errors.
- Legal disputes can arise from improper verification of provider qualifications.
- Ensure all delegated staff are trained and aware of compliance standards.
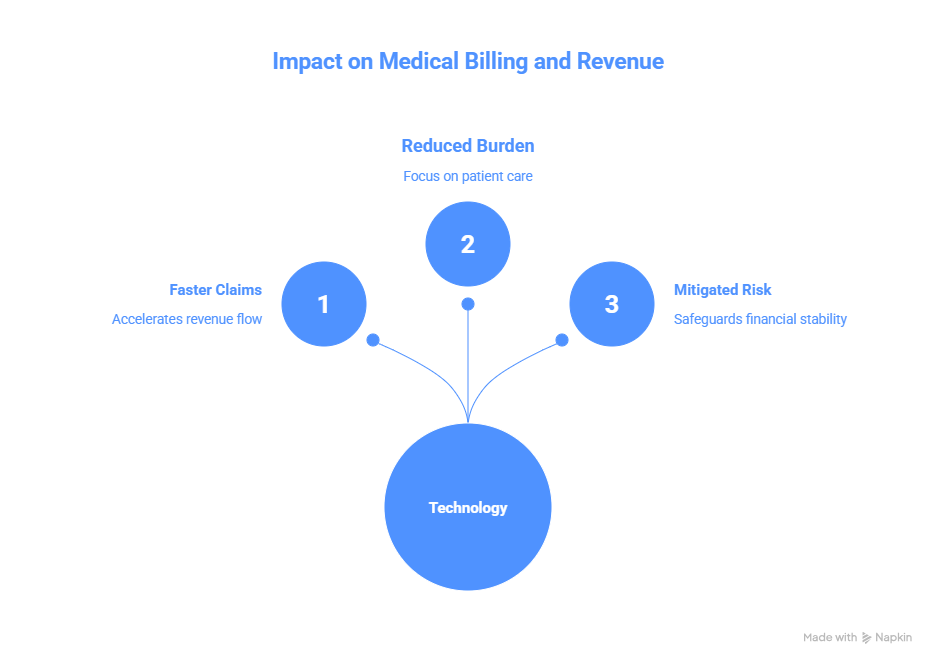
Impact on Medical Billing and Revenue Cycle
This section explains how delegated credentialing affects billing workflows and revenue cycle management. Proper implementation reduces claim delays and protects cash flow.
Faster Claims Processing
Delegated credentialing accelerates provider enrollment, ensuring claims are submitted with verified credentials. This reduces the risk of initial denials and speeds up reimbursements.
Key Points:
- Verified provider data allows immediate claim submission.
- Reduces rejected claims due to credentialing errors.
- Supports timely payer adjudication and faster payment cycles.
Reduced Administrative Burden
By delegating credentialing tasks, organizations can focus resources on billing, coding, and collections instead of verification work.
Key Points:
- Less duplicate data entry for billing staff.
- Fewer follow-ups for credential verification delays.
- Allows revenue cycle teams to prioritize accounts receivable management.
Mitigating Financial Risk
Errors in credentialing directly impact revenue. Delegated credentialing with proper oversight reduces compliance risks, minimizes claim denials, and secures consistent revenue flow.
Key Points:
- Prevents revenue loss from delayed provider approvals.
- Reduces exposure to payer audits and reimbursement disputes.
- Improves financial reporting and cash flow predictability.
When Delegated Credentialing Is Appropriate
This section highlights the scenarios where delegated credentialing provides value. It helps organizations reduce delays, optimize workflows, and improve compliance.
Large Healthcare Systems and Hospitals
Delegated credentialing is effective for hospitals and multi-provider health systems that manage high volumes of providers.
Key Points:
- Supports faster onboarding for dozens or hundreds of providers.
- Reduces duplicate credentialing across multiple departments.
- Allows internal teams to focus on quality and compliance oversight.
Organizations with Adequate Resources
Delegated credentialing requires infrastructure and personnel for audits, compliance, and reporting.
Key Points:
- Internal teams must monitor delegated entities and ensure NPDB checks.
- Credentialing software and standardized processes improve accuracy.
- Suitable for practices that can sustain ongoing oversight obligations.
Network Expansion and Timely Reimbursement Needs
When rapid enrollment and faster revenue flow are priorities, delegation is advantageous.
Key Points:
- Speeds provider approval for insurance panels.
- Minimizes claim denials from incomplete credentialing.
- Ensures revenue cycle efficiency and reduces accounts receivable delays.
Conclusion
When used with clear monitoring and compliance controls, delegated credentialing can greatly speed up provider onboarding and improve revenue cycle performance. Healthcare companies can lower claim denials and safeguard financial stability by coordinating their resources, auditing procedures, and delegated agreements.
Credentialing professionals, billing teams, and administrators can distribute tasks efficiently by knowing the difference between delegated and non-delegated credentialing. Effective management promotes timely patient treatment and effective revenue flow while guaranteeing following to NPDB, NCQA, and payer standards.
FAQs
What is delegated credentialing in healthcare?
Delegated credentialing allows a healthcare entity to assign another organization to verify provider qualifications. The delegating entity remains legally responsible for compliance.
How does delegated credentialing differ from non-delegated credentialing?
Delegated credentialing transfers verification tasks to a third party, shortening enrollment timelines. Non-delegated credentialing is handled entirely by the payer, often taking 90–120 days.
What compliance risks exist in delegated credentialing?
Mistakes in verification, NPDB reporting, or missed deadlines can trigger audits and claim denials. Delegating entities retain ultimate legal and financial liability.
How does delegated credentialing impact medical billing and the revenue cycle?
Proper delegated credentialing ensures accurate provider data for claims submission. This reduces denials, accelerates reimbursements, and improves cash flow.
When is delegated credentialing appropriate for a healthcare organization?
It suits large networks, hospitals, or organizations with sufficient resources for oversight. It ensures faster onboarding while maintaining compliance and accuracy.